2.1 Advocates for clients who have been neglected or underrepresented in the system.
During my time at an inpatient rehab facility, I often encountered clients who had been in hospitals for an extended amount of time. During this time, their medical needs took top priority as they faced challenges with being medically stable. Once they were stable and ready for rehabilitation to return to their home environment, their time would consist of gaining the strength and tolerance to safely return home. However, during these periods of time, their mental health was often not a priority over their other medical needs. I began to notice that many of my clients had not been outdoors and were experiencing signs of depression from being inside a hospital for such an extended amount of time. After noticing clients’ needs for their mental health to be addressed, I became more intentional with incorporating these needs into treatment sessions. One example of how I did this was by taking clients outside during their therapy sessions so they could feel the fresh air and sunshine. Pictured below is a discussion post about a specific time I addressed a client’s need that had been overlooked for so long.
During my time at an inpatient rehab facility, I often encountered clients who had been in hospitals for an extended amount of time. During this time, their medical needs took top priority as they faced challenges with being medically stable. Once they were stable and ready for rehabilitation to return to their home environment, their time would consist of gaining the strength and tolerance to safely return home. However, during these periods of time, their mental health was often not a priority over their other medical needs. I began to notice that many of my clients had not been outdoors and were experiencing signs of depression from being inside a hospital for such an extended amount of time. After noticing clients’ needs for their mental health to be addressed, I became more intentional with incorporating these needs into treatment sessions. One example of how I did this was by taking clients outside during their therapy sessions so they could feel the fresh air and sunshine. Pictured below is a discussion post about a specific time I addressed a client’s need that had been overlooked for so long.
|
2.2 Fulfills commitments to the professional community.
While completing my second level II rotation at an inpatient rehab facility, I had many opportunities to be involved with the professional community and attend various meetings. I was able to attend one of the weekly fall meetings where leaders within the facility discuss falls that occurred during the week and what could have been done to prevent the fall and utilize those ideas in the future. I attended a meeting that occurs daily where a representative from each discipline within the facility meets to discuss the current patient population and unique needs that may be present. I attended weekly meetings with the rehab staff where the director presented monthly fall rates, percentage of missed minutes with clients, satisfaction scores from discharged clients, and any other updates if applicable.
I also had the opportunity to shadow individuals from different disciplines within the facility such as a speech language pathologist (SLP), physical therapist (PT), medical doctor (MD), and nurse practitioner (NP). While shadowing an SLP, I had the opportunity to see VitalStim electrotherapy, and I shadowed a PT for a day to see more lower body treatments and long distance ambulation. I also had the opportunity to shadow one of the facility’s medical doctors and his nurse practitioner. I completed rounds with them, saw what they did behind the scenes, and was even asked to provide updates on clients’ progress with therapy if they were on my caseload. Through shadowing these different professions, I was able to see different aspects of care that clients receive and gained a better understanding of how different professionals work together in this setting. Pictured below is an exemplary performance score from my fieldwork educator about professional competence.
While completing my second level II rotation at an inpatient rehab facility, I had many opportunities to be involved with the professional community and attend various meetings. I was able to attend one of the weekly fall meetings where leaders within the facility discuss falls that occurred during the week and what could have been done to prevent the fall and utilize those ideas in the future. I attended a meeting that occurs daily where a representative from each discipline within the facility meets to discuss the current patient population and unique needs that may be present. I attended weekly meetings with the rehab staff where the director presented monthly fall rates, percentage of missed minutes with clients, satisfaction scores from discharged clients, and any other updates if applicable.
I also had the opportunity to shadow individuals from different disciplines within the facility such as a speech language pathologist (SLP), physical therapist (PT), medical doctor (MD), and nurse practitioner (NP). While shadowing an SLP, I had the opportunity to see VitalStim electrotherapy, and I shadowed a PT for a day to see more lower body treatments and long distance ambulation. I also had the opportunity to shadow one of the facility’s medical doctors and his nurse practitioner. I completed rounds with them, saw what they did behind the scenes, and was even asked to provide updates on clients’ progress with therapy if they were on my caseload. Through shadowing these different professions, I was able to see different aspects of care that clients receive and gained a better understanding of how different professionals work together in this setting. Pictured below is an exemplary performance score from my fieldwork educator about professional competence.
|
2.3 Represents the unique perspective of occupational therapy when participating in inter-professional situations.
During my rotation at West TN Rehab Hospital, I had the opportunity to participate in weekly team conferences. During these meetings, all members of the rehab team (OT, PT, SLP), medical doctors, lead nurse, and case managers are present to discuss the progress and needs of each client. For each client on our caseload, I would provide the team with the client’s level of progress, if they had impediments, if pain was interfering with therapy sessions, if they would need durable medical equipment (DME) or adaptive equipment (AE) at discharge, and what level they were functioning at for transfers and self-care tasks. By participating in these meetings, I was able to provide the OT perspective for each client’s needs. In doing this, other professionals became aware of client's occupational needs and could contribute their services to the client’s unique care. For example, if a client was having difficulty with pain during therapy sessions, the nurse and/or doctor could arrange for appropriate medication to be administered prior to therapy sessions. Pictured below is a discussion post where I explained my role in team conferences.
During my rotation at West TN Rehab Hospital, I had the opportunity to participate in weekly team conferences. During these meetings, all members of the rehab team (OT, PT, SLP), medical doctors, lead nurse, and case managers are present to discuss the progress and needs of each client. For each client on our caseload, I would provide the team with the client’s level of progress, if they had impediments, if pain was interfering with therapy sessions, if they would need durable medical equipment (DME) or adaptive equipment (AE) at discharge, and what level they were functioning at for transfers and self-care tasks. By participating in these meetings, I was able to provide the OT perspective for each client’s needs. In doing this, other professionals became aware of client's occupational needs and could contribute their services to the client’s unique care. For example, if a client was having difficulty with pain during therapy sessions, the nurse and/or doctor could arrange for appropriate medication to be administered prior to therapy sessions. Pictured below is a discussion post where I explained my role in team conferences.
|
2.4 Assumes responsibility for professional behavior and growth, in accordance with AOTA standards.
In accordance with AOTA standards, continued competence is imperative for carrying out the roles and abilities of an OT. To take responsibility for my professional growth during both of my level II rotations, I made sure I was prepared to administer assessments that my educators reported were often used at their facilities. For my pediatric rotation, I reviewed developmental milestones, the Sensory Profile 2, the Bruininks-Oseretsky Test of Motor Proficiency (BOT-2), and the Peabody Developmental Motor Scales (PDMS-2). After reviewing these, I made a reference sheet with key information to look back on if needed. As I reviewed for my inpatient rehab rotation, I made a similar reference sheet with manual muscle test (MMT) scores, GG scores, and notes for the Function in Sitting Test (FIST), Minnesota Manual Dexterity Test, and various precautions for the client population. Pictured below are some of the reference sheets that I made for myself as I prepared for fieldwork placements.
In accordance with AOTA standards, continued competence is imperative for carrying out the roles and abilities of an OT. To take responsibility for my professional growth during both of my level II rotations, I made sure I was prepared to administer assessments that my educators reported were often used at their facilities. For my pediatric rotation, I reviewed developmental milestones, the Sensory Profile 2, the Bruininks-Oseretsky Test of Motor Proficiency (BOT-2), and the Peabody Developmental Motor Scales (PDMS-2). After reviewing these, I made a reference sheet with key information to look back on if needed. As I reviewed for my inpatient rehab rotation, I made a similar reference sheet with manual muscle test (MMT) scores, GG scores, and notes for the Function in Sitting Test (FIST), Minnesota Manual Dexterity Test, and various precautions for the client population. Pictured below are some of the reference sheets that I made for myself as I prepared for fieldwork placements.

|

|
2.5 Functions autonomously and effectively in a broad array of service models.
During both of my fieldwork placements, my fieldwork educators eased me into taking on their caseloads. For both rotations, I was seeing an entire caseload by week 6, treating each client independently, and asking for assistance from my fieldwork educator when needed. Each day, I reviewed each client's chart and generated individual treatment ideas. During sessions, if the treatments I had planned were not appropriate for the client or not challenging enough, I would adapt my plan accordingly. For example, I evaluated a client who had experienced a stroke and planned to use electrical stimulation with functional activity during his sessions. However, as I observed his movements during sessions, I realized that he had functional muscle activation and was having difficulty with motor planning. I adapted his treatment plan to incorporate activities that challenged motor planing rather than muscle activation. I carried out his adapted treatment plan until he discharged from the facility. Throughout my inpatient rehab rotation, I had multiple opportunities to evaluate a client, develop a treatment plan, carry out the plan, and see them to the end of their care for discharge. Treating clients from the beginning to the end allowed me to build my confidence as a practitioner and meet productivity standards of an OT practitioner. Below is a comment from my fieldwork educator where she discussed my ability to function autonomously and take responsibility for clients' progress.
During both of my fieldwork placements, my fieldwork educators eased me into taking on their caseloads. For both rotations, I was seeing an entire caseload by week 6, treating each client independently, and asking for assistance from my fieldwork educator when needed. Each day, I reviewed each client's chart and generated individual treatment ideas. During sessions, if the treatments I had planned were not appropriate for the client or not challenging enough, I would adapt my plan accordingly. For example, I evaluated a client who had experienced a stroke and planned to use electrical stimulation with functional activity during his sessions. However, as I observed his movements during sessions, I realized that he had functional muscle activation and was having difficulty with motor planning. I adapted his treatment plan to incorporate activities that challenged motor planing rather than muscle activation. I carried out his adapted treatment plan until he discharged from the facility. Throughout my inpatient rehab rotation, I had multiple opportunities to evaluate a client, develop a treatment plan, carry out the plan, and see them to the end of their care for discharge. Treating clients from the beginning to the end allowed me to build my confidence as a practitioner and meet productivity standards of an OT practitioner. Below is a comment from my fieldwork educator where she discussed my ability to function autonomously and take responsibility for clients' progress.

|
2.6 Upholds the AOTA Code of Ethics in practice.
During both of my level II fieldwork rotations, I was responsible for sensitive client information. During my pediatric rotation, I was responsible for reviewing client history forms completed by parents as I wrote evaluation reports. After completing reports, I would dispose of the documents per facility policy. While at West TN Rehab Hospital, I would receive a print out of the daily schedule, which included clients’ names, birthday, and room number. At the end of each day, I would place my schedule in the appropriate disposal bin provided by the facility. Along with properly disposing documents with client information at both facilities, I was intentional about not using clients’ names in public areas when speaking with other professionals. At the inpatient rehab facility, it was common to refer to clients by their room number when speaking with other members of their care team. By adhering to these measures, I was able to uphold AOTA Code of Ethics in many areas, specifically in areas of Justice and Dignity. Pictured below is an exemplary performance score and comment provided by my fieldwork educator regarding my ability to adhere to AOTA’s Code of Ethics.
During both of my level II fieldwork rotations, I was responsible for sensitive client information. During my pediatric rotation, I was responsible for reviewing client history forms completed by parents as I wrote evaluation reports. After completing reports, I would dispose of the documents per facility policy. While at West TN Rehab Hospital, I would receive a print out of the daily schedule, which included clients’ names, birthday, and room number. At the end of each day, I would place my schedule in the appropriate disposal bin provided by the facility. Along with properly disposing documents with client information at both facilities, I was intentional about not using clients’ names in public areas when speaking with other professionals. At the inpatient rehab facility, it was common to refer to clients by their room number when speaking with other members of their care team. By adhering to these measures, I was able to uphold AOTA Code of Ethics in many areas, specifically in areas of Justice and Dignity. Pictured below is an exemplary performance score and comment provided by my fieldwork educator regarding my ability to adhere to AOTA’s Code of Ethics.
|
2.7 Serves as a role model for honesty, integrity, and morally grounded decision making.
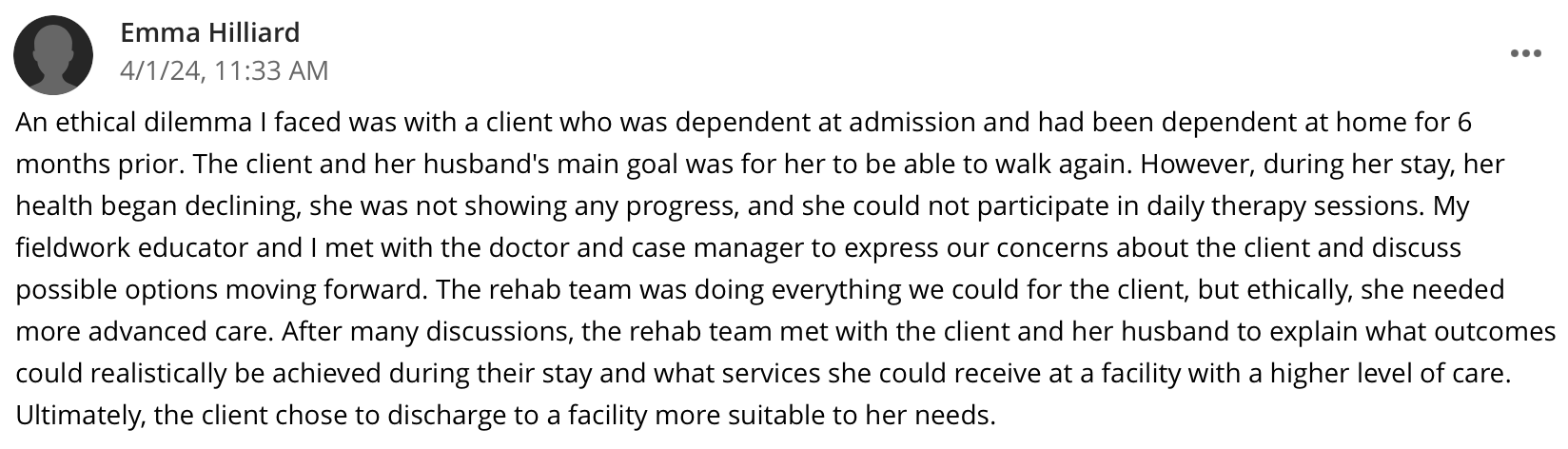
As an OT practitioner, it is important to be a positive role model for others while practicing honesty, integrity, and making morally ground decisions. I demonstrated these qualities during both of my fieldwork placements. One way I maintained these qualities at West TN Rehab Hospital was by participating in team conferences and providing honest information when deciding where a client should discharge to, how long they will need at the rehab hospital, and what equipment they would need. One particular time that required a great level of honesty and integrity was with a client who was not making progress during her time at the rehab hospital and needed additional care that was beyond what the facility could provide for her. My fieldwork educator and I took necessary actions to discuss these concerns with the rest of the team and advocate for the client’s needs. Pictured below is a discussion post where I explained this situation in further detail.
As an OT practitioner, it is important to be a positive role model for others while practicing honesty, integrity, and making morally ground decisions. I demonstrated these qualities during both of my fieldwork placements. One way I maintained these qualities at West TN Rehab Hospital was by participating in team conferences and providing honest information when deciding where a client should discharge to, how long they will need at the rehab hospital, and what equipment they would need. One particular time that required a great level of honesty and integrity was with a client who was not making progress during her time at the rehab hospital and needed additional care that was beyond what the facility could provide for her. My fieldwork educator and I took necessary actions to discuss these concerns with the rest of the team and advocate for the client’s needs. Pictured below is a discussion post where I explained this situation in further detail.
|
