1.1 Appreciates the influence of socio-cultural, socioeconomic, political, diversity factors, and lifestyle choices on engagement in occupation throughout the lifespan.
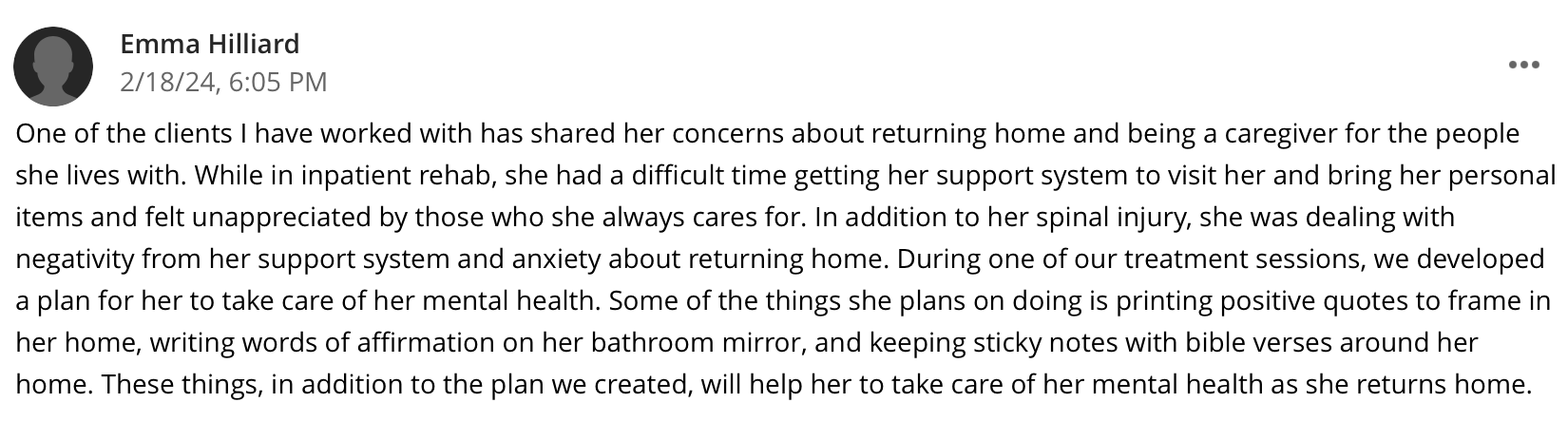
During my time at West TN Rehab Hospital, I had the privilege of encountering individuals from many walks of life. When evaluating clients, my fieldwork educator encouraged me to get to know the client on a deeper level, find out what they do to occupy their time, ask questions about their life before they were admitted to the hospital, and discuss what their life would look like when they were discharged. By having these conversations from the beginning, I was able to learn more about the client’s background and have a better understanding of where they came from. Having this deeper understanding allowed me to develop treatment plans specific to the client’s needs and their unique factors. One example of how I considered a client’s cultural factors and lifestyle choices on engagement in occupation was with a client who lived with her siblings and was the main caretaker for the household. She expressed concerns about her previous lifestyle, returning home to take care of others, and was concerned about her mental health as she returned to her unique environment. Pictured below is a discussion post where I explained how I incorporated the client’s concerns into her treatment plan, as well as a picture of how my fieldwork educator scored my performance with respecting diversity factors.
During my time at West TN Rehab Hospital, I had the privilege of encountering individuals from many walks of life. When evaluating clients, my fieldwork educator encouraged me to get to know the client on a deeper level, find out what they do to occupy their time, ask questions about their life before they were admitted to the hospital, and discuss what their life would look like when they were discharged. By having these conversations from the beginning, I was able to learn more about the client’s background and have a better understanding of where they came from. Having this deeper understanding allowed me to develop treatment plans specific to the client’s needs and their unique factors. One example of how I considered a client’s cultural factors and lifestyle choices on engagement in occupation was with a client who lived with her siblings and was the main caretaker for the household. She expressed concerns about her previous lifestyle, returning home to take care of others, and was concerned about her mental health as she returned to her unique environment. Pictured below is a discussion post where I explained how I incorporated the client’s concerns into her treatment plan, as well as a picture of how my fieldwork educator scored my performance with respecting diversity factors.

|
|
1.2 Communicates effectively with a wide range of clients, peers, and professionals both verbally and non-verbally.
During both of my level II fieldwork placements, I was required to effectively communicate with many different individuals. During my time at Janna Hacker and Associates (pediatric setting), I was tasked with communicating with children in a way they could understand, as well as communicating with parents to explain what their child’s session consisted of and how each activity/task was beneficial to their child’s growth in developmental milestones, social skills, problem solving skills, handwriting skills, etc. I became more confident in communicating the OT reasoning behind tasks when speaking with parents and discussing how their child performed. I continued using these skills as I began my fieldwork rotation at the West TN Rehab Hospital. I communicated effectively with clients, caregivers, and other professionals. I was able to communicate the importance of OT and discuss clients’ progress with caregivers and other healthcare professionals. Pictured below is a comment from my fieldwork educator explaining my progress with becoming more comfortable communicating the OT process, as well as my exemplary performance score for articulating the value of OT.
During both of my level II fieldwork placements, I was required to effectively communicate with many different individuals. During my time at Janna Hacker and Associates (pediatric setting), I was tasked with communicating with children in a way they could understand, as well as communicating with parents to explain what their child’s session consisted of and how each activity/task was beneficial to their child’s growth in developmental milestones, social skills, problem solving skills, handwriting skills, etc. I became more confident in communicating the OT reasoning behind tasks when speaking with parents and discussing how their child performed. I continued using these skills as I began my fieldwork rotation at the West TN Rehab Hospital. I communicated effectively with clients, caregivers, and other professionals. I was able to communicate the importance of OT and discuss clients’ progress with caregivers and other healthcare professionals. Pictured below is a comment from my fieldwork educator explaining my progress with becoming more comfortable communicating the OT process, as well as my exemplary performance score for articulating the value of OT.

|
1.3 Collaborates with clients and caregivers in establishing and maintaining a balance of pleasurable, productive, and restful occupations to promote health and prevent disease and disability.
My second level II fieldwork site was a certified stroke facility, and my fieldwork educator led one of the stroke teams, so I had many opportunities to interact with clients who had experienced a stroke. In addition to therapy sessions, these clients received various forms of stroke education. Through education groups, as well as during daily therapy sessions, I discussed risks, signs, and symptoms of a stroke, as well as educate clients on beneficial changes to make after having a stroke. I assisted with educating clients and caregivers on healthy food choices, benefits of daily activity and exercise, and provide tips for maintaining awareness of their health. I encouraged clients to attend doctor appointments regularly, take medications as prescribed, limit fried food consumption, drink plenty of water, and record their blood pressure twice a day. Through educating clients and caregivers on life after a stroke, I informed them on how to maintain a balanced lifestyle for improved health and prevention of an additional stroke or further disease. Linked below is a PDF format of the booklet we used during stroke education groups at West TN Rehab Hospital.
https://encompasshealth.com/-/media/healthsouth/project/healthsouth/files/life_after_stroke_07_19.pdf
My second level II fieldwork site was a certified stroke facility, and my fieldwork educator led one of the stroke teams, so I had many opportunities to interact with clients who had experienced a stroke. In addition to therapy sessions, these clients received various forms of stroke education. Through education groups, as well as during daily therapy sessions, I discussed risks, signs, and symptoms of a stroke, as well as educate clients on beneficial changes to make after having a stroke. I assisted with educating clients and caregivers on healthy food choices, benefits of daily activity and exercise, and provide tips for maintaining awareness of their health. I encouraged clients to attend doctor appointments regularly, take medications as prescribed, limit fried food consumption, drink plenty of water, and record their blood pressure twice a day. Through educating clients and caregivers on life after a stroke, I informed them on how to maintain a balanced lifestyle for improved health and prevention of an additional stroke or further disease. Linked below is a PDF format of the booklet we used during stroke education groups at West TN Rehab Hospital.
https://encompasshealth.com/-/media/healthsouth/project/healthsouth/files/life_after_stroke_07_19.pdf
1.4 Inspires confidence in clients and team members.
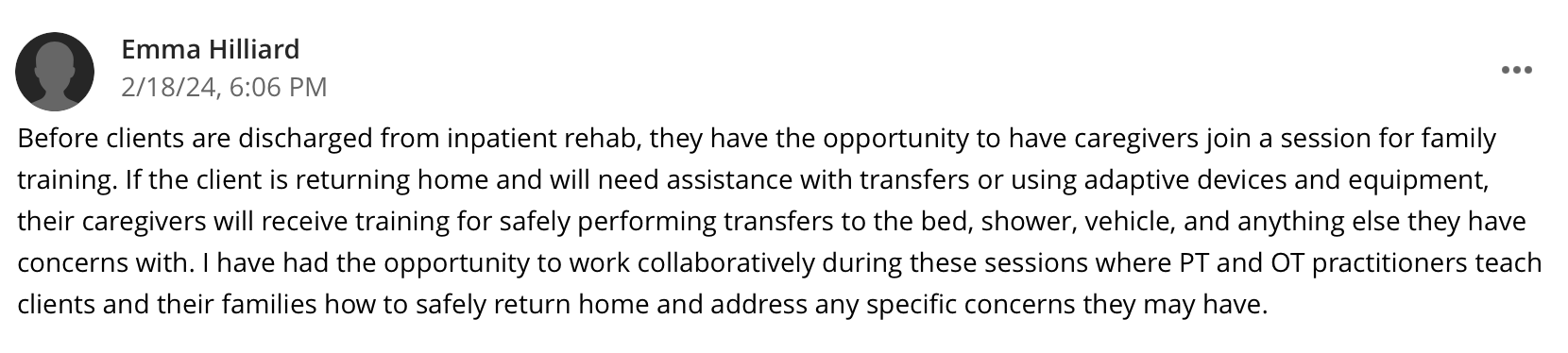
During my rotation at West TN Rehab Hospital, I had the opportunity to be a cheerleader for clients when they weren’t confident in themselves. Oftentimes when a client would be nervous about safely returning home, I would encourage them and discuss the progress they made during their rehab stay. I found that it was beneficial to refer back to the client’s level of function at admission to reiterate how many skills they have accomplished. I would also explain that the rehab team would not recommend the client return to home if they were not going to be safe and have the support they needed. After having these conversations, clients would be more confident in themselves and recognize the progress they had made. I would also participate in family training and family conferences, which would provide an opportunity for client’s caregivers to attend sessions and learn more about caring for their loved one. Through this opportunity, clients and caregivers became more confident in returning home together and performing daily tasks. Pictured below is a discussion post where I explained family training sessions.
During my rotation at West TN Rehab Hospital, I had the opportunity to be a cheerleader for clients when they weren’t confident in themselves. Oftentimes when a client would be nervous about safely returning home, I would encourage them and discuss the progress they made during their rehab stay. I found that it was beneficial to refer back to the client’s level of function at admission to reiterate how many skills they have accomplished. I would also explain that the rehab team would not recommend the client return to home if they were not going to be safe and have the support they needed. After having these conversations, clients would be more confident in themselves and recognize the progress they had made. I would also participate in family training and family conferences, which would provide an opportunity for client’s caregivers to attend sessions and learn more about caring for their loved one. Through this opportunity, clients and caregivers became more confident in returning home together and performing daily tasks. Pictured below is a discussion post where I explained family training sessions.
|
1.5 Considers client motivation when using occupation-based intervention to maximize functional independence.
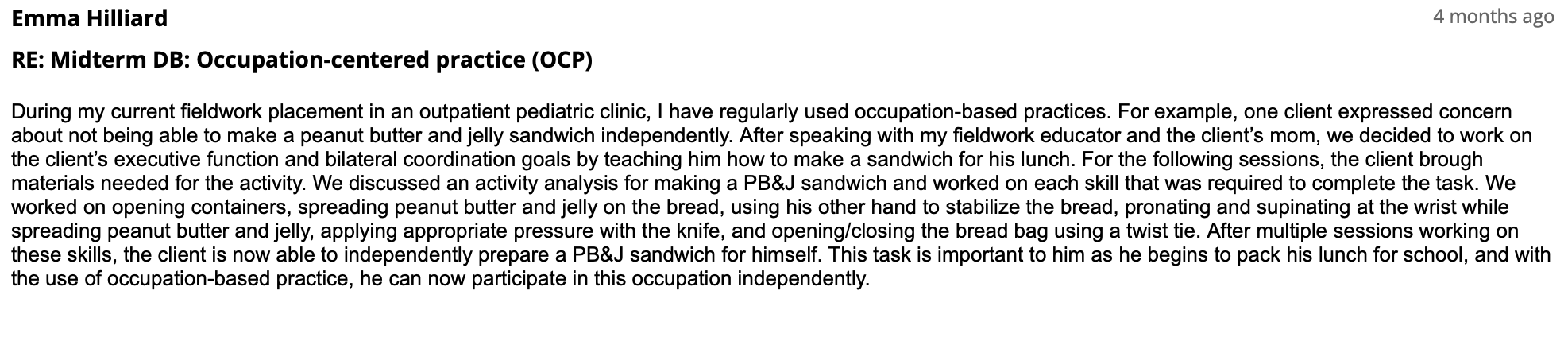
In the field of occupational therapy, it is important for practitioners to use occupation as a means to an end. One of my favorite ways I have incorporated an occupation into a session to maximize functional independence was during my pediatric rotation at Janna Hacker and Associates. One of the clients had goals for executive function and bilateral coordination, and he expressed concern for not being able to make a sandwich. We used the activity of preparing a sandwich to work towards his OT goals. Pictured below is a discussion post where I further explained how this client’s desire to be able to make a sandwich was used as an occupation-based intervention.
In the field of occupational therapy, it is important for practitioners to use occupation as a means to an end. One of my favorite ways I have incorporated an occupation into a session to maximize functional independence was during my pediatric rotation at Janna Hacker and Associates. One of the clients had goals for executive function and bilateral coordination, and he expressed concern for not being able to make a sandwich. We used the activity of preparing a sandwich to work towards his OT goals. Pictured below is a discussion post where I further explained how this client’s desire to be able to make a sandwich was used as an occupation-based intervention.
|
1.6 Applies theory regarding the therapeutic use of occupation and adaptation to screen and evaluate, plan, and implement intervention, while establishing and maintaining a therapeutic relationship with the client.
Although an occupational profile is not separately filled out during evaluations at most facilities, I find it important to still gather the necessary information from the client that would complete their occupational profile. By doing this, I am able to form a more therapeutic relationship with the client, find out what their life looks like, learn what is important to them, and identify potential areas of their daily life to incorporate into OT interventions. Even if multiple clients have the same goals, it is important to form therapeutic relationships with them so that their intervention plan is unique to their individual needs and interests.
Digging deeper into the clients’ personal life and interests is one way I have used theories like the Person-Environment-Occupation model (PEO). During my rotation at West TN Rehab Hospital, I was able to gain this information during evaluations by asking the client about their home life, who they live with, how many stairs they have at home, how their bathtub/shower is set-up, how much assistance they required for activities of daily living (ADLs) prior, what they did to occupy their time, etc. Based on how the client answered these questions, I was able to develop a treatment plan to meet their needs to return to their home environment safely. Pictured below is a proficient performance score from my fieldwork educator about how I managed therapeutic relationships with my clients.
Although an occupational profile is not separately filled out during evaluations at most facilities, I find it important to still gather the necessary information from the client that would complete their occupational profile. By doing this, I am able to form a more therapeutic relationship with the client, find out what their life looks like, learn what is important to them, and identify potential areas of their daily life to incorporate into OT interventions. Even if multiple clients have the same goals, it is important to form therapeutic relationships with them so that their intervention plan is unique to their individual needs and interests.
Digging deeper into the clients’ personal life and interests is one way I have used theories like the Person-Environment-Occupation model (PEO). During my rotation at West TN Rehab Hospital, I was able to gain this information during evaluations by asking the client about their home life, who they live with, how many stairs they have at home, how their bathtub/shower is set-up, how much assistance they required for activities of daily living (ADLs) prior, what they did to occupy their time, etc. Based on how the client answered these questions, I was able to develop a treatment plan to meet their needs to return to their home environment safely. Pictured below is a proficient performance score from my fieldwork educator about how I managed therapeutic relationships with my clients.

|
